Rapidly locate the patient.
Reach them faster.
Get them to the right hospital.
912Rwanda
912Rwanda is an end-to-end emergency dispatch system that locates patients, coordinates response, and optimizes hospital decision and routing in Rwanda. "We used to rely on guesswork and phone calls;now everything is digital, and we save lives faster" — SAMU driver, interview with Rwanda Health Magazine, September 2025
The Challenges
Emergency deaths in LMICs are often driven not only by lack of access, but by lack of coordination.
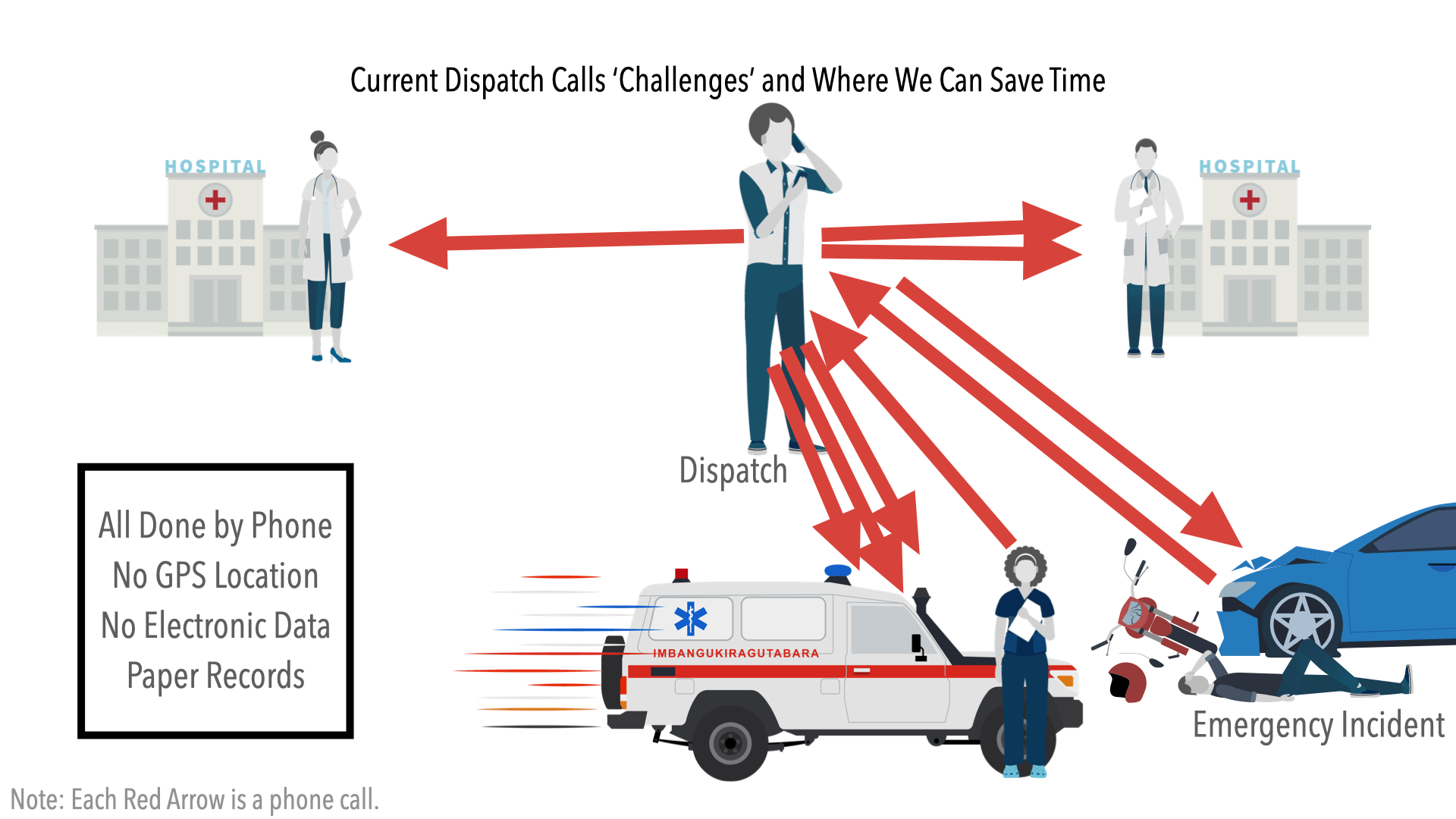
47% of injury-related deaths in Kigali occur before hospital arrival, while many conventional dispatch platforms are poorly suited for the Kigali context and hilly road structure, where formal addresses, reliable connectivity, and standardized infrastructure cannot be assumed. In such environments, delays in locating the scene, dispatching the right ambulance, communicating with field teams, and routing patients to an appropriate facility can be fatal. 912Rwanda was developed with SAMU to address these failures directly through a digitally coordinated emergency response platform designed for Rwanda's real operating conditions.
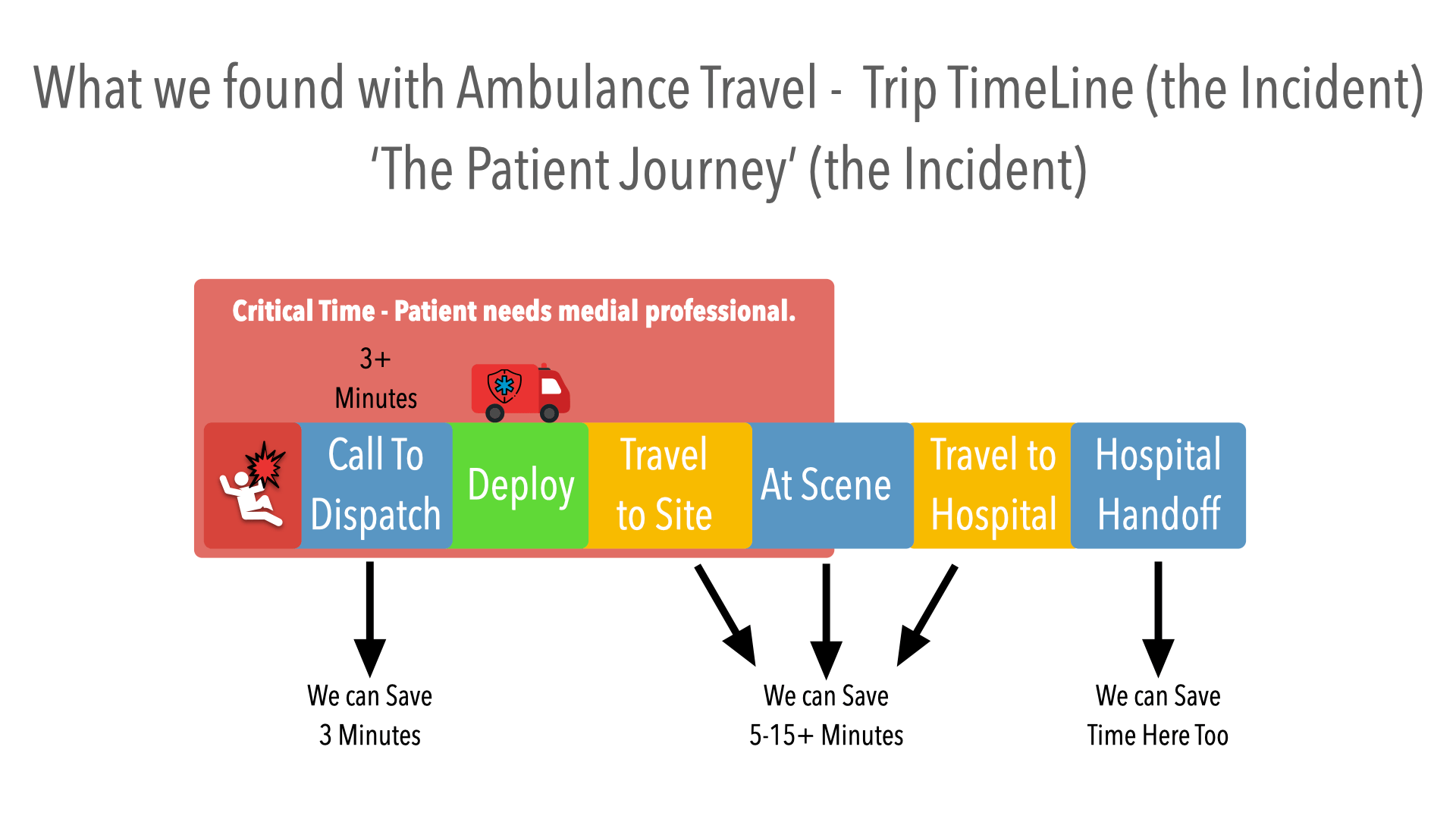
During the 2018–2020 discovery phase, a critical operational bottleneck was identified in locating the patient. On average, more than three minutes of each emergency call were spent clarifying the patient's location, followed by an additional 5 to 15 minutes of ambulance travel and on-scene search time to accurately find the incident. These delays were compounded by downstream inefficiencies, with approximately 20% of patient handoffs requiring diversion to a secondary facility, reflecting gaps in initial routing and system-wide coordination.
912Rwanda as the Solution
Ambulance Team Dispatch and Trip Tracking Foundation
912Rwanda was designed and used as Rwanda’s national emergency medical dispatch and coordination platform
Designed and developed for Rwanda
Developed by the Rwanda Build Program (RWBuild), in partnership with the Ministry of Health (MOH), Rwanda Biomedical Center (RBC), and SAMU, with support from the University of Utah Global Health program and the University of Birmingham, the system was designed to address a fundamental challenge in LMIC emergency response: locating patients, coordinating care, and routing them efficiently to the appropriate facility in real time.
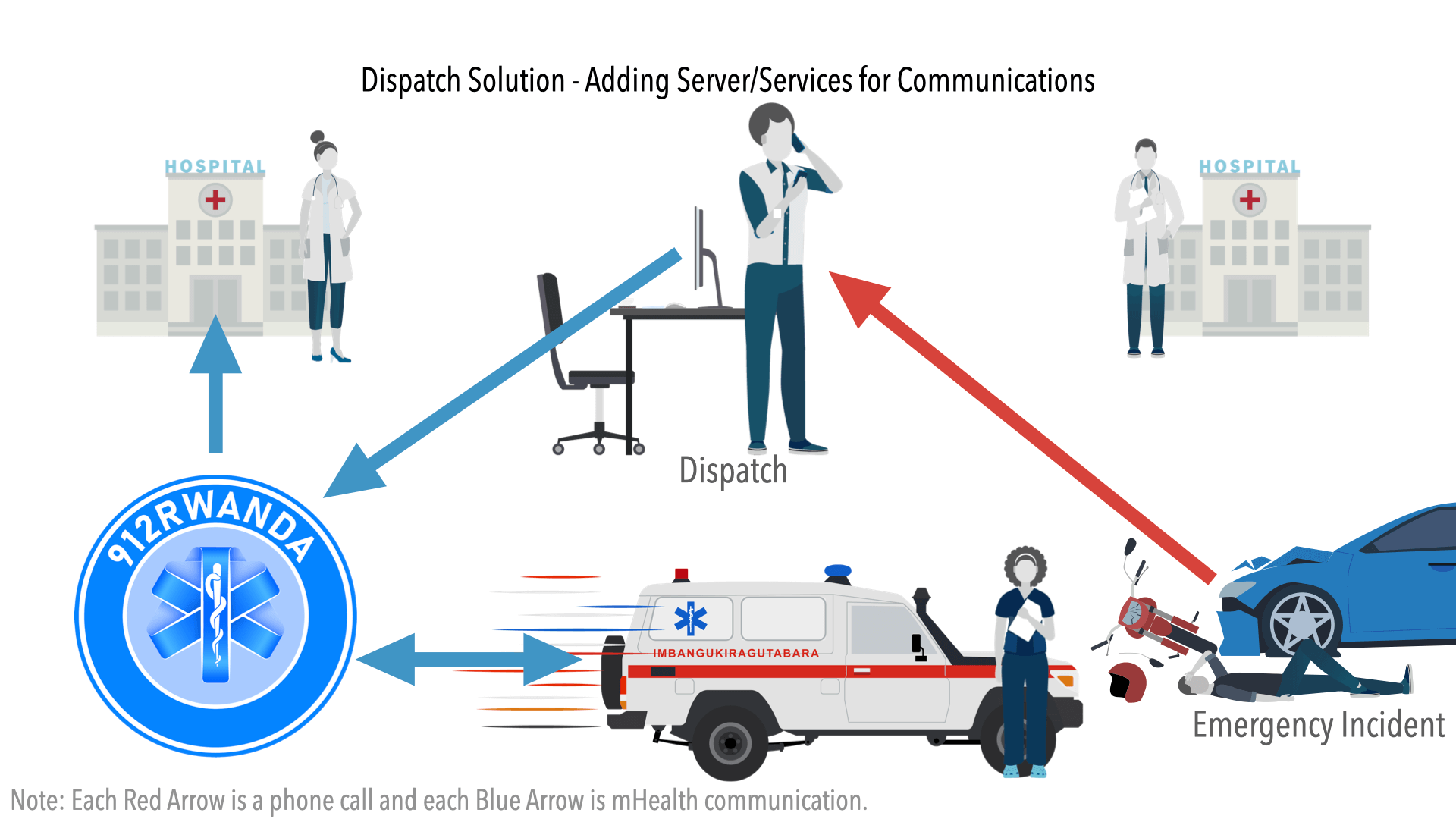
Unified Command
Since its inception in 2018, 912Rwanda has been built through a structured, multi-year collaboration grounded in operational realities. The platform replaces fragmented, phone-based coordination with a unified, digital command system that enables dispatchers, ambulance teams, and hospitals to operate as a single coordinated network. It ensures that the right ambulance reaches the exact location and that each patient is transported to the most appropriate facility—efficiently, reliably, and at the right time
Globally Funded & Tested
With over $5 million in funding from leading global health institutions, including the U.S. National Institutes of Health (NIH) and the UK National Institute for Health and Care Research (NIHR), 912Rwanda has been rigorously developed, tested, and deployed over a seven-year period. Every core feature was co-designed and validated with SAMU leadership, ensuring alignment with national workflows, clinical needs, and real-world operating conditions. The result is a scalable, field-tested system that transforms emergency response into a coordinated, data-driven service—improving response times, strengthening clinical decision-making, and enabling governments to operate modern, efficient emergency medical systems at a national level.
Comprehensive Project Phases
This phase established the foundation for 912Rwanda through close collaboration between RWBuild, SAMU (under the Ministry of Health and RBC), and international experts. Field discovery and early prototypes focused on understanding real operational constraints — particularly patient location, dispatch delays, and coordination gaps. A software prototype was funded by the VCU School of Medicine.
During this phase, RWBuild developed and deployed a pre-launch data collection application and service for SAMU, funded by the U.S. National Institutes of Health (Fogarty International Center). This enabled real-world data capture, workflow validation, and iterative refinement of system design. The outputs of this phase directly informed the architecture, use cases, and evidence base required for large-scale funding and national deployment. The data was also useful to SAMU for refining their workflows.
With Funding from the US NIH (National Institute of Health Fogarty Institute), a partnership with the Rwanda Biomedical Center / Ministry of Health, and Dr. Sudha Jayaraman with the University of Utah Center for Global Surgery, this phase focused on developing the foundational function and wider services for dispatch and ambulance focused on deployment to reduce time. Communication and tracking to ensure SAMU reaches the patient rapidly. This phase began a new era in emergency response efficiency in Rwanda.
Launched August 2023 (updates and iterations added every month until 2025) Funded by the U.S. National Institutes of Health (Fogarty International Center), and implemented in partnership with RBC/MOH and the University of Utah Health, this phase delivered the core national dispatch platform. Phase 1 focused on replacing fragmented, phone-based coordination with a centralized digital command system that includes real-time ambulance tracking, dispatch management, and structured incident workflows. The system was deployed operationally with SAMU, validating end-to-end functionality from call intake through ambulance deployment to hospital handoff, and establishing the national digital foundation for emergency response.
Launched August 2025 (updates and features added in 2026) Supported by the UK National Institute for Health and Care Research (NIHR) and led by the University of Birmingham and broader Rwandan institutional partners, this phase expands the system into advanced clinical coordination and decision support. Phase 2 introduces structured patient data capture in the field, facility readiness tracking, and intelligent routing that matches patients with the most appropriate hospital. These capabilities transform 912Rwanda from a dispatch system into a fully coordinated, data-driven emergency care platform—optimizing outcomes by ensuring patients are located, treated, and transported to the right facility at the right time.
Impact Measurement and Reporting
912Rwanda operates as a fully data-driven national system, capturing every stage of the emergency response — from call intake and patient location to dispatch, transport, and hospital handoff. The platform measures key performance indicators, including response times, deployment metrics, location accuracy, journey efficiency, and facility routing outcomes. Real-time dashboards provide national visibility, enabling continuous operational improvement and more effective resource planning.
This structured data approach supports both day-to-day decision-making and long-term policy development, while enabling formal evaluation with global health partners. Early results show clear gains in coordination and response efficiency.
Key Features — Phase 1 & Phase 2
Phase 1 — Ambulance Team Dispatch and Trip Tracking Foundation
Centralized command, resilient offline design, and real-time ambulance coordination.
- Centralized, role-based digital dispatch command center
- Real-time ambulance tracking and deployment management
- Advanced location mapping with community geolocation (works without formal addresses)
- Pre-deploy alerts to accelerate ambulance mobilization
- Dynamic diversion and reassignment of vehicles in real-time
- End-to-end delay tracking and operational performance monitoring
- Mobile field app for ambulance teams (navigation, secure communication, incident logging)
- Structured incident and journey tracking (call → dispatch → transport → handoff)
- Real-time dashboards for SAMU and MOH operational visibility
- Offline-capable design tuned for Rwanda's connectivity constraints
Phase 2 — Clinical Coordination & System Intelligence
Structured clinical workflows, facility readiness, and intelligent routing.
- Structured patient data capture in the field with guided workflows
- Facility readiness tracking (beds, staffing, capability)
- Destination Decision Support (DDSA) for optimal hospital routing
- Automated hospital pre-notification with ETA and patient summary
- Advanced data reporting and analytics for national planning
- Deeper integration and coordination between dispatch, field teams, and receiving hospitals
The Importance of Academic and Government Partnerships
The success of 912Rwanda reflects nearly a decade of sustained partnership between RWBuild, the SAMU division of the Ministry of Health (MOH), the Rwanda Biomedical Center (RBC), global health experts, and international academic institutions. Academic partners — the University of Birmingham and the University of Utah Health — have played a critical role in scientific rigor, evaluation frameworks, and alignment with global best practices in emergency care.
Each core feature of 912Rwanda was designed in full collaboration with SAMU. Features began as core needs identified during discovery, and SAMU gave final approval before development. This stakeholder loop included guidance from international partners and global health experts, ensuring that 912Rwanda would be both useful and impactful to Rwanda's pre-hospital care.
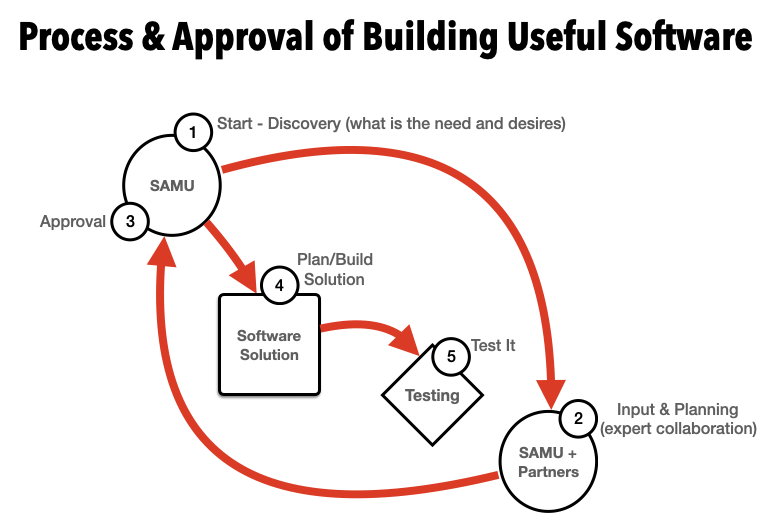
The original concepts were written and presented, generating multiple letters of agreement and tested to two of the Rwanda MOUs. This long-term partnership model — combining government leadership, local implementation, and academic validation — has been essential to building a system that is not only functional, but credible, scalable, and impactful.
Partners
Media Links
Publications on 912Rwanda
Slide Solutions
Gallery